Rethinking RA outcome prediction
SUMMARY
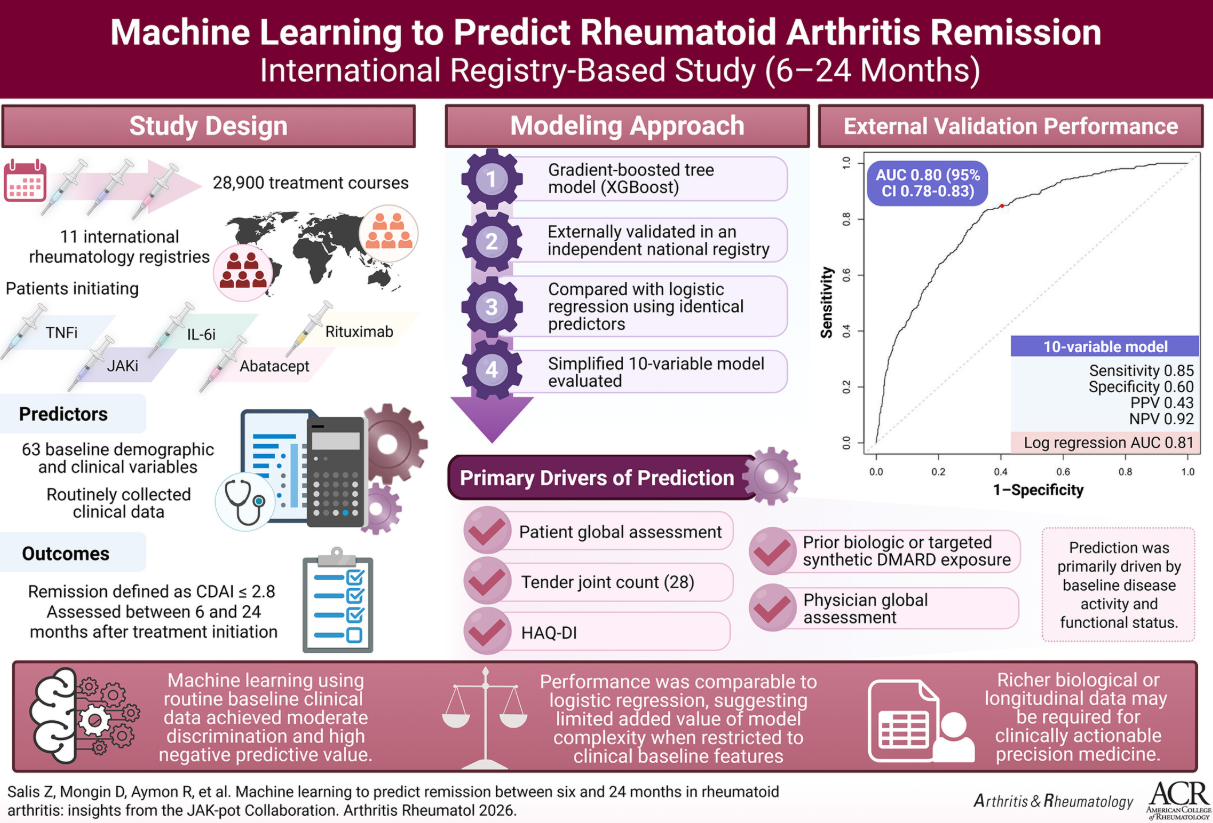
The authors developed, externally validated, and simplified a machine-learning (ML) model to predict remission between six and 24 months in rheumatoid arthritis (RA) patients initiating TNF inhibitors, JAK inhibitors, IL-6 inhibitors, abatacept, or rituximab, using data from 11 international registries in the JAK-pot collaboration.
They analyzed 21,675 treatment courses for model training, 5,418 courses for internal validation, and 1,807 courses from Switzerland for external validation. Remission was defined as a Clinical Disease Activity Index (CDAI) ≤2.8 within six to 24 months after treatment initiation or switching. An XGBoost model was trained on 63 baseline demographic and clinical variables. Model performance was evaluated using the area under the curve (AUC), sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Predictor contributions were quantified using SHAP values. A simplified model using the top ten predictors and a logistic regression benchmark were also evaluated.
In external validation, the full model achieved an AUC of 0.797 (95% CI: 0.774–0.821), sensitivity of 0.804, specificity of 0.650, PPV of 0.454, and NPV of 0.902. The simplified model performed comparably (AUC: 0.802). Logistic regression using the same ten predictors achieved an AUC of 0.809. Key predictors included patient global assessment, 28-tender joint count, previous biologic/tsDMARD exposure, and HAQ-DI.
Using routinely collected baseline data across 11 registries, prediction of remission showed limited discrimination and was best suited to ruling out remission. Performance was similar for a ten-variable model and logistic regression, indicating limited incremental value of model complexity without richer predictors.
Full article: https://doi.org/10.1002/art.70165
WHY IS THIS IMPORTANT?
This study investigated whether machine learning could help improve predicting which patient will reach remission in rheumatoid arthritis patients starting advanced therapies. Using real-world data from multiple countries, the model showed only modest predictive performance, and was better at identifying patients unlikely to improve substantially. Unexpectantly, traditional statistical methods performed similarly. This suggests that current clinical data used for decision-making may not capture all the factors involved in reaching remission. For the wider population, this matters because it demonstrates the limitations of current methods used to predict clinical outcomes and emphasises the need for better data, in particular novel biomarkers, to truly personalise treatment and improve long-term outcomes in RA.
20 Apr 2026